")



Place Matters Oregon/PMO: First of all, thank you so much for being our first guest for the Place Matters Oregon (PMO) blog. Will you tell us a bit about your background and your work?
West: Before I started at Oregon Health & Science University (OHSU), I worked in Guatemala as the maternal and child health program coordinator for Medical Teams International, a non-governmental nonprofit based in Portland. That’s where my interest in public health and community health began. That’s also where my journey toward spinal cord injury began when I was hit by a truck and broke my hip. I was flown to a U.S. hospital for surgery. During my course of care, I acquired a hospital-infection in my spine. Ten days later I woke up in the ICU paralyzed. This definitely galvanized my focus. I finished my public health degree at OHSU and have worked in disability and the health system. Around 2015 I started a nonprofit called the Oregon Spinal Cord Injury Connection that promotes health, builds community, and creates opportunities for people with spinal cord injuries in Oregon and SW Washington.

Currently, I work at the Oregon Office on Disability and Health at OHSU where I enjoy advocating for systems-level change that contributes to Oregon’s health care transformation efforts. I advocate for policies and systems- and environmental-changes that make healthy choices and access to health care easier for people with disabilities.
PMO: Can you give us an example of your work?
West: Sure. I am a member of the Health Equity Committee of the Oregon Health Policy Board. We review and propose policies that advance health equity. One of our recent achievements was recommending a definition of health equity that OHA adopted. The definition includes people with disabilities, which might seem obvious, but it wasn’t too long ago when state and federal public health entities weren’t even collecting data on people with disabilities. This definition will have downstream impacts across OHA and the state.
PMO: What are the major barriers that people with disabilities face? From our work creating the new Place Matters Oregon videos now on the website, we understand there are physical barriers, but there are also more invisible barriers. And all of these barriers have an impact on disparities for chronic disease. Would you tell us about the physical barriers first?
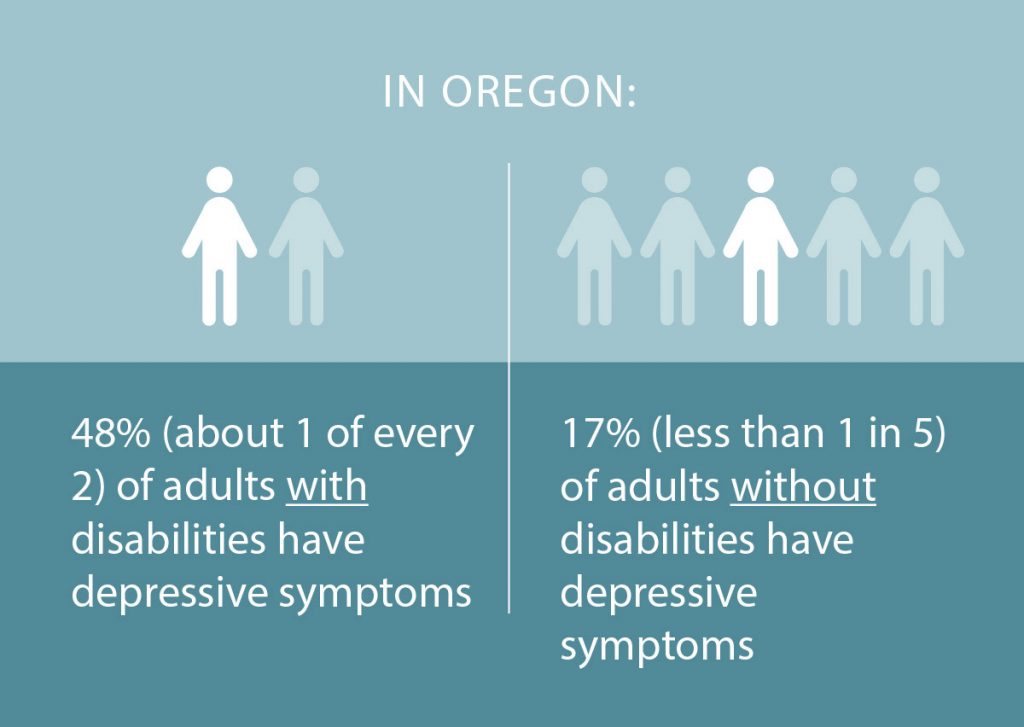
West: People living in Oregon with disabilities are 3x more likely to report having diabetes, over 4x more likely to report having heart disease, twice as likely to be physically inactive in the last 30 days and nearly 2.5x more likely to report being depressed than Oregonians without disabilities. For the most part, these health conditions are preventable and aren’t a result of one’s disability. As a person with a disability, I encounter multiple physical barriers every day that impede my ability to be active and participate in society. As an example, if a person with a physical disability wants to participate in an exercise program at the gym, they will likely encounter numerous barriers. They may find impassable sidewalks, bus stops or street crossings, or face a lack of accessible, affordable, convenient public transportation. The gym may not be accessible, or may not have adapted equipment or trained staff to support adaptive exercise activities. This may be especially true in more rural areas or economically depressed areas of Oregon. There is exclusion at every level. People with a disability actually can and do exercise; it’s not that they choose not to but for many it’s an access issue.
These barriers contribute to Oregonians with disabilities being less physically active. And if these are barriers a person with a disability faces going to the gym, imagine how physical barriers inhibit a person’s ability to access health care. We know being less active due to physical barriers, or any barriers for that matter, can contribute to having a higher BMI, which can contribute to diabetes. This is, in fact, what we see among Oregonians with disabilities. They are less likely to be physically active, more likely to develop diabetes, and more likely to rate their health as poor or fair than their able-bodied counterparts. Physical barriers also contribute to social isolation and depression, as well as a significantly higher prevalence of chronic diseases for people living with disabilities. This example illustrates how physical and built environment barriers can contribute to the prevalence of chronic disease among Oregonians with disabilities.
PMO: And now let’s move to those more invisible barriers, things that are social and cultural, right? What is your perspective on this, particularly since you not only work in this field, but you are experiencing it yourself?
West: OK, I’ll use another example. It’s mind boggling to me that these systemic barriers against people with disabilities still exist. Medicaid asset income restrictions, which are set by the Centers for Medicaid and Medicare, unjustly penalize workers with a disability who need long-term supports and services. In order to be eligible for long-term supports and services through Medicaid, a person in Oregon with a disability must limit their countable assets to $5,000 and income to less than 250% of the Federal Poverty Level, which is $32,000 for a family of 1 or $55,000 for a family of 3. By restricting a disabled employee’s ability to earn and save, the state has closed all pathways to prosperity in the best- case scenario, and indentured that family to poverty in more difficult circumstances. That person can never take a pay raise, even if they merit it, without risking losing their health benefits.
These policies are regressive and discriminatory against people with disabilities. Imagine if your private health insurance payer dramatically restricted your income and assets in exchange for covering your cholesterol medication. Undoubtedly, we’d think that is unfair. This is the situation some Oregon workers with disabilities face. Because they need long-term supports and services, like a personal care attendant to help them with the activities of their life, they are forced to live on restricted assets and income. And unfortunately, no other private or employee-based insurance will pay for a round-the-clock personal care attendant to support a worker with a disability. It’s not the person with a disability’s fault, but Oregon’s Medicaid asset and income eligibility requirements discriminate against them, barring them from fully participating in gainful employment or advancing in their jobs. The downstream effect of these policies is it’s harder for people with disabilities to advance into management, upper management or executive positions. These restrictions need to be removed, but without people with disabilities in positions of power, it’s even harder for us to make systemic change.

Other invisible challenges include attitudinal barriers, or stigma against people with a disability. People who live with disabilities are more likely to be victims of violence than those without disabilities. Attitudinal barriers also inform our cultural norms, values, stories and images. There are no movies with superheroes who are disabled; people living with a disability are not portrayed as sexy or attractive. If you have a disability, you can feel unwelcome and treated as “other” from media, magazines and culture. Those all inform what it means to be disabled. People with disabilities have strengths just like others, and improving media representation with positive images and narratives, like what the Paralympics has done, will continue to help combat stigma.
I’m married. It’s not uncommon for people to say to my wife, “you’re brave” to have married someone with disabilities. Their biases, their attitudinal barriers, lead to discrimination.
PMO: Employment is one huge area where stigma is a challenge for people living with disabilities. What are some common misconceptions—about work or daily life—that you’d like to share and correct for people reading this?
West: One common misunderstanding is that productivity and creativity have to follow a uniform process, say working 9 to 5 in an office. Now with COVID-19 and all of our technology, many people are working from home, and productivity and creativity seem to be working out. Interestingly, this may make it easier for people living with a disability to work because when working from home a person can safeguard their health while also remaining productive. If I can manage my own work schedule from home, it’s so much easier. I can be on a computer screen and it doesn’t matter where I am. While the work-from-home situation is more optimal and may facilitate more people with disabilities working, I don’t think it will eliminate stigma against disability.

PMO: This year – 2020 – is the 30th anniversary of the Americans with Disabilities Act (ADA). Since we’re talking about how place affects health at Place Matters Oregon, share your own perspective on how the ADA has shaped places over the last 30 years and made them more accessible to people with disabilities.
West: I would divide up the ADA’s contributions into two categories–physical access and communications access. Let’s look at physical changes first. These include disability parking requirements; an accessible path of travel from parking to the front door, into common areas, like restrooms; requirements for wheelchair access that include ramped or level entrances, doorway width requirements, specific door hardware, accessible restrooms, accessible tables, desks and benches; and more accessible counters, kiosks and self-service stations. Really, universal design benefits us all—think of people like a mother with a stroller, who now has an easier time taking a walk because of curb cuts on sidewalks. And communication access means required signage for way-finding; and provision of some auxiliary aids and services in state and local government programs.
The bottom line—better access equals inclusion and participation for all. And it’s good to have perspective. In December, I went to Mexico City with my wife. The U.S. is not perfect but if you’ve ever traveled with anyone in a wheelchair in another country, it’s really easy to notice the absence of things like uniform curb cuts or ramps that aren’t ridiculously steep. Airplane travel is not great but it’s getting better. ADA parking close to a building has probably kept me alive, because a wheelchair user is really hard to see behind an SUV when it’s backing out of a spot. It’s not just for convenience but safety. While the ADA is not perfect, we’ve made progress as a country and have a foundation that we can continue to improve upon.
The Oregon Department of Parks & Recreation is a great example of a state agency trying to make things more inclusive. They have the right spirit as they work on improving trails, campsites and boat ramps. That innovation warms my heart and gives me hope.

PMO: What else would you like people to know about living with a disability, or the connection of place and health in supporting people with disabilities?
West: I’m really pleased that OHA decided to collaborate with OODH on this project. To me, it represents a first step of acknowledging meaningful change in policies, systems and programs to make Oregon more inclusive and accessible. The valuable nugget in all of this is that Oregon is ready to change, people are ready—they want to be more inclusive; they want to learn. From a professional perspective, I was humbled. We’re together and united in wanting to make change.
Connect with West on LinkedIn: https://www.linkedin.com/in/west-livaudais-mph-65842559 or by email: livaudai@ohsu.edu.
West Livaudais works at the Oregon Office on Disability and Health (OODH), a public health program under the Institute on Development and Disability at the Oregon Health & Science University (OHSU).
![]() This is the first guest blog by Place Matters Oregon – to find out more go to: https://placemattersoregon.com/
This is the first guest blog by Place Matters Oregon – to find out more go to: https://placemattersoregon.com/
Let’s make more healthy places for us all. Place Matters Oregon is an initiative of the Oregon Health Authority. Our goals are to foster conversations among Oregonians about how place affects health and to inspire collective action that will make a healthy life available to all people in our state. Together, we can create more opportunities for every Oregonian—no matter what town or city we call home—to live a long, healthy life.
https://placemattersoregon.com/blog/a-personal-story-about-making-oregon-more-inclusive/